
Last Updated: October 30, 2025
Introduction to Argininosuccinate Lyase Deficiency
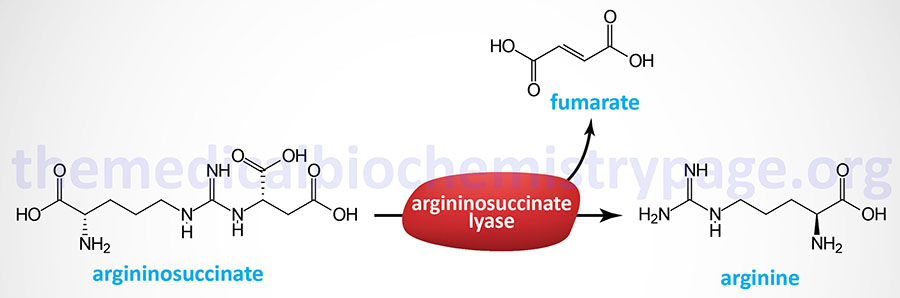
As the name implies, argininosuccinate lyase deficiency (ALD) is a disorder resulting from mutations in the gene (ASL) encoding the urea cycle enzyme, argininosuccinate lyase. Argininosuccinate lyase catalyzes the hydrolysis of argininosuccinate into arginine and fumarate.
The inheritance of ALD is autosomal recessive and occurs with a frequency of approximately 1 case per 70,000 live births. Argininosuccinate lyase deficiency results in accumulation and urinary excretion of argininosuccinate and as such this disorder is commonly referred to as argininosuccinic aciduria.
Molecular Biology of Argininosuccinate Lyase Deficiency
Argininosuccinate lyase (AL) is also called argininosuccinase. Argininosuccinate lyase is encoded by the ASL gene. The ASL gene is located on chromosome 7q11.21 and is composed of 16 exons that generate four alternatively spliced mRNAs. These four mRNAs give rise to three different isoforms of the AL enzyme. AL isoform 1 is 464 amino acids, isoform 2 is 444 amino acids, and isoform 3 is 438 amino acids. The functional AL enzyme exists as a homotetramer.
The human AL protein is highly similar (60%) to avian and reptilian crystalin proteins of the lens. Examination of mutations in the AL gene that give rise to argininosuccinate lyase deficiency (ALD) from 28 patients has identified at least 12 allelic mutations. Mutations include missense and nonsense mutations, exon deletions, and splice site variants.
Clinical Consequences of Argininosuccinate Lyase Deficiency
ALD is, like the other neonatal onset forms of onset urea cycle disorders (UCD), most severe when presenting in newborn infants. As with each of the four neonatal onset UCD, ALD is characterized by the accumulation of ammonia and glutamine with clinical manifestations appearing in full-term infants with no prior obstetric risk factors. The classic symptoms appear between 24hrs and 48hrs after birth (but not prior to 24hrs) and include convulsions, hyperventilation, ataxia, hypothermia, lethargy, vomiting and poor feeding. If left untreated the hyperammonemia with result in coma and death. The severe effects of hyperammonemia are described in the Nitrogen Metabolism page. Even though sepsis is a rare event in a normal term infant with no prior obstetric complications, this disorder is misdiagnosed in almost half of neonatal UCD cases.
Initial laboratory findings will include respiratory alkalosis which is the earliest objective indication of encephalopathy. The encephalopathy will progress to the point where mechanical ventilation is required. Another routine laboratory finding is reduced serum (blood) urea nitrogen (BUN) which may be as low as 1mg/dl (normal for newborns is 3–12mg/dl). If plasma ammonia levels are not measured the infants’ death will be attributed to sepsis, intracranial hemorrhage, or some other disorder that would normally be associated with a pre-term delivery.
Treatment of Argininosuccinate Lyase Deficiency
ALD patients are treated in much the same ways as for other neonatal UCDs in that protein intake must me highly regulated and the hyperammonemia must be controlled. Hemodialysis is the only effective means to rapidly lower serum ammonia levels in these patients. Acute episodes of hyperammonemia can be treated with intravenous administration of Ammunol® and with oral Buphenyl® for chronic adjunctive therapy of hyperammonemia. The mechanism of action of these compounds is detailed in the Urea Cycle Disorders: Overview page.
Treatment of ALD patients with large amounts oral arginine aids in waste nitrogen removal. The oral arginine is converted to urea and ornithine via the arginase reaction of the urea cycle. The ornithine (along with carbamoyl phosphate) is then converted to citrulline through the action of ornithine transcarbamylase (OTC). Citrulline is then converted to argininosuccinate via the argininosuccinate synthetase reaction which also requires aspartate. The net effect is that nitrogen in carbamoyl phosphate and arginine is eliminated as argininosuccinate.